Obsessive-Compulsive Disorder and the Need for Control in Everyday Life
Obsessive-Compulsive Disorder and the Need for Control in Everyday Life
1.1 When Control Becomes a Burden
1.2 Obsessive Thoughts and Compulsive Actions
1.3 The Difference Between Conscientiousness and Compulsion
How Does the Compulsion to Check Manifest Itself in Everyday Life?
2.1 Typical Situations Involving Compulsive Checking
2.2 Impact on Work, Family and Social Contacts
Causes and Psychological Dynamics of Obsessive-Compulsive Disorder
3.1 Biological and Psychological Factors
3.2 Why Are Obsessive Thoughts So Persistent?
3.3 The Role of Responsibility and Perfectionism
3.4 Stress as a Trigger
Why Compulsions Cannot Simply Be “Switched Off”
4.1 The Compulsion Cycle
4.2 Reassurance and Avoidance
4.3 When Is Professional Help Advisable?
Treatment of Obsessive-Compulsive Disorder at the LIMES Schlossklinik Bergisches Land
6.1 Is a Strong Need for Control Always an Obsessive-Compulsive Disorder?
6.2 Can You Get Rid of Obsessive Thoughts by Suppressing Them?
6.3 Can Obsessive-Compulsive Disorder Still Be Treated Even After Many Years?
Obsessive-Compulsive Disorder and the Need for Control in Everyday Life
Obsessive-compulsive disorder can significantly alter everyday life. What initially appears to be an increased need for security, order or control often develops into a distressing cycle of inner tension, recurring thoughts and ritualised behaviours for those affected. In international usage, the condition is often referred to as OCD, derived from ’Obsessive Compulsive Disorder’.
Typically, those affected usually recognise their thoughts or actions as excessive or unreasonable. Nevertheless, they are unable to permanently refrain from these compulsions. If a control ritual is not performed, this often leads to severe anxiety, fear, disgust, feelings of guilt or the sense of having failed to prevent a potential danger.
When Control Becomes a Burden
Control is, initially, a normal human need. It helps us assess risks, take responsibility and organise daily life reliably. It becomes problematic when it can no longer be used flexibly, but instead seems absolutely necessary.
A pronounced need for control can manifest itself, for example, in repeatedly checking doors, repeatedly checking electrical appliances or reviewing work documents again despite having checked them carefully. What is decisive here is not merely the action itself, but the inner pressure behind it. If checking no longer brings peace of mind but instead generates new doubts, this may indicate a compulsion to check.
Obsessive Thoughts and Compulsive Actions
Obsessive-compulsive disorders often consist of two closely linked elements: obsessive thoughts and compulsive actions. Obsessive thoughts are recurring, intrusive thoughts, images or impulses that are experienced as unpleasant, shameful or threatening. They do not occur voluntarily and are often difficult to suppress.
Compulsive actions are repeated behaviours or mental rituals intended to reduce tension or prevent a feared consequence. These include, for example:
- repeated checking of doors, windows or hob rings
- excessive washing or cleaning
- constant ordering, counting or repeating
- mentally checking whether something was done wrong
- seeking reassurance from other people
In the short term, these actions may provide relief. In the long term, however, they reinforce the cycle of compulsion because the brain learns that safety seems possible only through the ritual.
The Difference Between Conscientiousness and Compulsion
Conscientiousness is associated with diligence, a sense of responsibility and reliability. Obsessive-compulsive disorder goes beyond this. It is not an expression of particular meticulousness, but rather a psychological burden that increasingly takes control of thoughts and actions.
Key differences are particularly evident in terms of inner freedom:
- Voluntariness: Conscientious people can consciously complete a task. With an obsessive-compulsive disorder, however, there is a feeling of having to check again.
- Proportionality: A normal check is proportionate to the situation. With compulsive checking, the action is repeated even though there is objectively no new reason to do so.
- Relief: Diligence brings clarity. Compulsive actions usually provide only brief reassurance before new doubts arise.
How Does the Compulsion to Check Manifest Itself in Everyday Life?
The compulsion to check can occur in many areas of life. It particularly often affects situations where responsibility, safety or potential mistakes play a role. Those affected then not only assess objective risks but also try to create an inner sense of absolute certainty. However, it is precisely this certainty that usually remains unattainable.
Typical Situations Involving Compulsive Checking
In everyday life, compulsive checking often manifests in seemingly trivial moments. This is precisely why it is long underestimated. Those affected often continue to function reliably on the outside, but internally require ever more energy to cope with their daily routines.
Typical situations may include:
- repeatedly checking whether the front door is locked
- checking whether the hob, iron or lights have been switched off
- rereading messages for fear of mistakes
- repeatedly checking medical symptoms
- worrying that one’s own behaviour may have endangered others
It is not uncommon for such checks to become part of fixed rituals. A door, for example, must then be checked not just once, but in a specific order or with a specific sense of inner certainty.
Impact on Work, Family and Social Contacts
Obsessive-compulsive disorder is rarely limited to individual actions. Over time, it can structure daily routines and restrict important areas of life. At work, this can lead to delays, concentration problems or excessive checking for errors. People with high levels of responsibility, in particular, often try to compensate for their symptoms for a long time.
The private sphere is also affected. Family members are asked for reassurance, joint appointments are delayed or everyday routines are disrupted by checking behaviours. At the same time, many of those affected feel ashamed of their compulsions and increasingly withdraw.
The consequences often manifest themselves in several areas:
- Time loss
Checking rituals prolong everyday routines, for example before appointments, before leaving the house or before going to sleep. - Concentration problems
Obsessive thoughts consume attention, making work, conversations or leisure activities more difficult. - Family tensions
Relatives are drawn into seeking reassurance or come under pressure to respect certain rituals. - Social withdrawal
Out of shame or exhaustion, those affected avoid meetings, travel or new situations.
This withdrawal can exacerbate the burden. The fewer opportunities there are for corrective experiences in daily life, the more firmly the conviction takes hold that control is necessary to establish a sense of security.
Causes and Psychological Dynamics of Obsessive-Compulsive Disorder
Obsessive-compulsive disorder is rarely caused by a single trigger. In most cases, biological, psychological and life history factors interact. Stress, stressful life events or periods of high responsibility can also contribute to the exacerbation of existing vulnerabilities.
Biological and Psychological Factors
At a biological level, changes in brain networks relevant to error detection, impulse control and emotional evaluation are among the factors discussed in relation to obsessive-compulsive disorder. Neurotransmitter systems, particularly serotonin and dopamine, may also play a role.
Psychologically, an exaggerated sense of responsibility is often at the forefront. Those affected overestimate the likelihood of negative events or perceive thoughts as morally significant. A thought such as “What if I’ve hurt someone?” is then not dismissed as a mere thought, but interpreted as an indication of a real danger.
Why Are Obsessive Thoughts So Persistent?
Obsessive thoughts are not distressing because they are particularly unusual. Many people experience fleeting, unpleasant or absurd thoughts.
However, with obsessive-compulsive disorder, these thoughts become overvalued. They trigger intense anxiety and are experienced as something that must be controlled, neutralised or refuted.
Paradoxically, the attempt to get rid of obsessive thoughts often makes them more present. The more strongly a thought is suppressed, the more attention it receives. This creates a cycle of observation, evaluation and renewed anxiety.
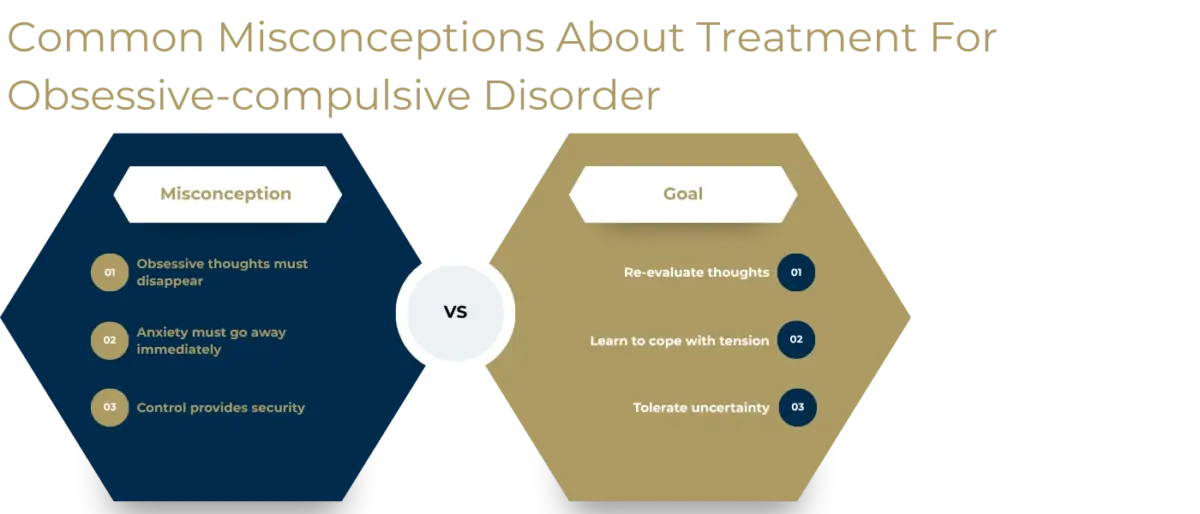
A different therapeutic approach to these thoughts is therefore helpful:
- Contextualising thoughts: An obsessive thought is initially an internal event, not evidence of a real danger.
- Changing evaluation: It is not the thought itself that is the main problem, but the significance attributed to it.
- Reducing rituals: If every unpleasant feeling is not immediately neutralised, the brain can store new experiences.
- Tolerating uncertainty: The aim is not absolute certainty, but a practical way of dealing with remaining uncertainty.
The Role of Responsibility and Perfectionism
Many people affected have high internal standards. Mistakes must be avoided at all costs, risks completely ruled out, and other people protected. These traits may initially appear as strengths in a professional or private context. In the context of an obsessive-compulsive disorder, however, they become a burden.
Perfectionism reinforces the impression that only absolute certainty is acceptable. A “probably everything is fine” is no longer enough. Instead, there is pressure to achieve a 100% sense of security. Yet it is precisely this feeling that cannot be forced.
Stress as a Trigger
Stress does not necessarily cause OCD, but it can significantly exacerbate its symptoms. During periods of high stress, the need for predictability increases. Checking behaviours then provide short-term structure and relief.
Typical triggers in everyday life can include:
- Performance pressure
High professional demands, examinations or personal commitments increase the need to rule out mistakes. - Family conflicts
Tensions in the environment can intensify inner uncertainty and encourage compulsions. - Changes
Relocations, career changes, separations or new phases of life can intensify checking rituals. - Lack of sleep
Exhaustion reduces mental resilience and makes obsessive thoughts harder to manage. - Isolation
When those affected have fewer stress-relieving activities, rumination and compulsive behaviour often increase.
Why Compulsions Cannot Simply Be ’Switched Off’
To outsiders, compulsive behaviours can sometimes seem baffling. However, simply telling someone to stop checking things does not go far enough. Obsessive-compulsive disorder is not a habit that can be overcome through sheer willpower. It is rooted in complex processes of anxiety and learning that require targeted therapeutic intervention.
The Compulsion Cycle
The compulsion cycle often begins with a trigger. This can be a situation, a thought or a physical sensation. This is followed by an assessment: something might be dangerous, wrong or irresponsible. This assessment creates tension.
The compulsive act reduces the tension in the short term. However, this is precisely what reinforces it. The brain registers that the relief was caused by the act of checking. The next time a similar trigger occurs, the ritual seems even more necessary.
Reassurance and Avoidance
Alongside visible checking behaviours, reassurance and avoidance play a central role. Those affected ask family members whether anything really happened, search the internet for confirmation or avoid situations that might trigger doubts.
These strategies are understandable, but they perpetuate the condition:
- Reassurance
The confirmation of others usually provides only brief relief. Afterwards, there is often a desire for further reassurance. - Avoidance
Difficult situations are no longer experienced. This means there are no opportunities to learn that anxiety can subside even without a ritual. - Mental checking
Those affected mentally replay situations over and over. This too can become an internal ritual. - Checking by family members
Family members sometimes take over checking behaviours. In the short term, this provides relief; in the long term, it maintains the compulsion.
When Is Professional Help Advisable?
Professional support is advisable when compulsions significantly impair time, quality of life or relationships. Even if those affected can conceal their symptoms, the inner psychological distress is often considerable.
Warning signs include:
- Checks or rituals take up a significant amount of time each day.
- Decisions are avoided out of fear of making mistakes.
- Family members are regularly involved in seeking reassurance.
- Work or personal commitments suffer as a result of the compulsions.
- Shame, withdrawal or depressive symptoms increase.
Early treatment can help break the cycle of compulsion before avoidance behaviour becomes further entrenched.
Treatment of Obsessive-Compulsive Disorder at the LIMES Schlossklinik Bergisches Land
At the LIMES Schlossklinik Bergisches Land, we treat Obsessive-Compulsive Disorder within a specialised, secure and high-quality therapeutic setting. The primary focus is on thorough psychiatric, psychological and psychosomatic diagnostics. Here, we look not only at the visible compulsion to check, but also at co-occurring burdens such as anxiety, depressive symptoms, sleep problems, psychosomatic complaints or stress-related exhaustion.
On this basis, an individually tailored treatment plan is developed. The aim is to understand the personal cycle of compulsion, professionally contextualise distressing obsessive thoughts and gradually develop new behavioural patterns. The focus is not on short-term symptom relief, but on long-term stabilisation and greater autonomy in everyday life.
Specific treatment options may include:
- Comprehensive diagnostics and personalised treatment plan
At the beginning of treatment, the type, intensity and function of the compulsions are carefully assessed. The results form the basis of a highly individualised treatment plan that takes account of the individual’s specific symptoms, co-morbid conditions and life circumstances. - High-frequency psychotherapy in individual and group sessions
Psychotherapeutic work forms the basis of the treatment. In individual sessions, specific obsessive thoughts, checking rituals and underlying cognitive patterns can be addressed in a nuanced way. Group therapy elements additionally facilitate discussion, contextualisation and relief. - Cognitive behavioural therapy and exposure therapy
In cases of obsessive-compulsive disorder, it can be therapeutically beneficial to gradually seek out triggering situations and refrain from performing habitual compulsive actions as before. In this way, those affected learn that tension can subside even without performing a control action. This process is structured, professionally supervised and individually tailored. - Specialised therapies for stabilisation
In addition to psychotherapy, relaxation and mindfulness exercises, physiotherapy and occupational therapy, as well as other therapeutic services, can be used. They support the regulation of inner tension, strengthen body awareness and help to develop alternative coping strategies. - LIMES Sports.Care
Physical activity can help reduce stress, clear the mind and strengthen the connection to the here and now. The clinic’s personalised sports concept is integrated into the holistic treatment plan and can effectively complement psychological stabilisation in cases of obsessive-compulsive disorder. - Healing Environment in a peaceful setting
The exclusive, safe and relaxing environment of the LIMES Schlossklinik Bergisches Land supports the therapeutic process. Taking a break from the stresses of everyday life can help break ingrained patterns and enable new experiences in dealing with uncertainty.
The treatment is designed not to reduce those affected to their symptoms. Instead, the focus is on the person behind the condition. The therapeutic aim is to reduce the influence of compulsions, build inner security and gradually regain greater freedom of action.
Find out more here about the range of therapies offered by our clinic.
FAQ
Is a Strong Need for Control Always an Obsessive-Compulsive Disorder?
No. A strong need for control is not automatically pathological. The key factor is whether the checking remains voluntary, appropriate and situation-specific. A possible obsessive-compulsive disorder is more likely to be diagnosed if repeated checking cannot be avoided despite knowing better, triggers intense internal pressure and noticeably restricts daily life.
Can You Get Rid of Obsessive Thoughts by Suppressing Them?
Consciously suppressing obsessive thoughts usually only helps in the short term or may even intensify them. Therapy is therefore not about preventing every thought. The aim is rather to change how the thoughts are evaluated and to attach less importance to them. As a result, they gradually lose their emotional power.
Can Obsessive-Compulsive Disorder Still Be Treated Even After Many Years?
Yes. Even long-standing obsessive-compulsive disorder can be treated. Although compulsions can become entrenched over the years, thought and behaviour patterns can still be changed through therapy. What is important is a thorough diagnosis, a personalised treatment plan and a willingness to gradually gain new experiences in dealing with uncertainty.
Kategorien: Obsessive-Compulsive Disorders
